
Post-Traumatic Stress Disorder (PTSD)
|
If you are interested in counseling for PTSD, call OakHeart at 630-570-0050 or 779-201-6440 or email us at [email protected]. We have counselors, psychologists, and social workers available to help you at one of our locations in North Aurora, IL, Sycamore, IL, and/or via Telehealth Online Therapy Services serving Kane County, DeKalb County, Dupage County, and beyond.
What is PTSD?PTSD can be an incredibly debilitating disorder that can create a lot of confusion, fear, frustration, and a sense of loss of ones identity. Many people have experienced, witnessed, or have heard about distressing or terrifying events. This does not necessarily result in the development of PTSD, as some are able heal without developing symptoms that impact their functioning. However, others are unable to heal on their own and may go on to develop PTSD.
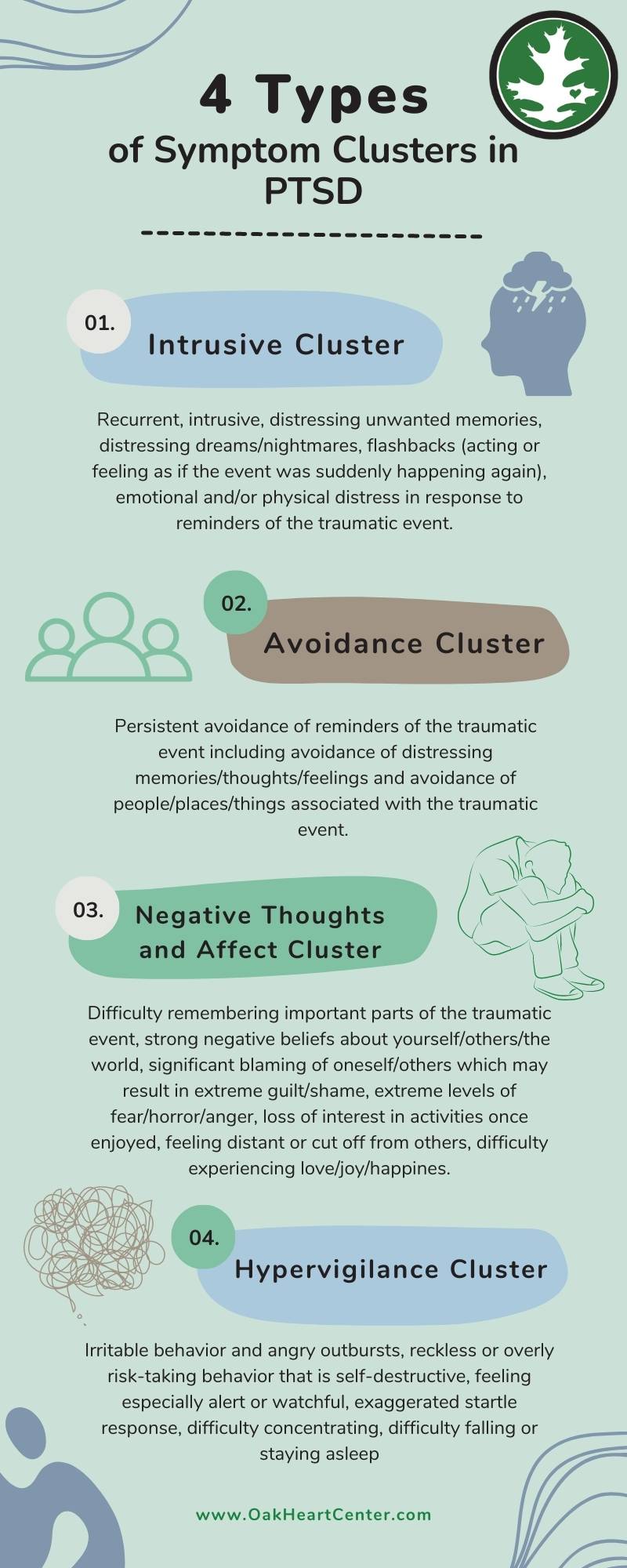
Someone who has PTSD was exposed to one or more of the following: death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence. These events may have occurred through being a witness, experiencing the trauma directly, witnessing a traumatic event, learning that a friend or relative experienced a trauma, or indirect exposure to averse details of trauma (i.e., occupations that involve exposure to traumatic situations). Individuals with PTSD re-experience the event in an intrusive and distressing manner (i.e., flashbacks, nightmares, upsetting memories, emotional or physical reactivity when confronted with reminders of the event). In order to cope, a person with PTSD may make attempts to avoid remembering trauma by refusing to think or feel in relation to the event or to be in situations that remind him/her/them of the event. Consequently, negative thoughts and/or feelings develop or become enhanced; such as blaming oneself for what happened, having negative thoughts about the self, others, and the world, feeling isolated, struggling to enjoy activities, and difficulty experiencing positive emotion. Lastly, a person’s arousal and reactivity changes, which can manifest as hypervigilance, irritability or aggression, risky or destructive behavior, trouble sleeping and/or concentrating, or heightened startle response.
|


|
These symptoms develop as a way to protect the body and self, because an individual’s system is perpetually in a state of fight-or-flight. It does this to constantly scan for threats, but in reality, it makes functioning very difficult. It is common for people with PTSD to experience issues with safety, trust, power and control, self-esteem, intimacy, their occupation, school, and relationships. They find their world getting smaller as their attempts to escape and avoid the trauma start affecting many aspects of their lives.
|
How do you Treat PTSD?There are many forms of treatment for PTSD and at OakHeart, we implement evidence-based therapies that have been shown to be clinically effective for this disorder. Specifically, we offer three treatment approaches: Cognitive-Processing Therapy (CPT), Prolonged Exposure Therapy (PE), and Emotion-Focused Therapy (EFT). Sometimes an integration of therapies can be helpful, depending on the needs of the client.
Cognitive Processing Therapy (CPT):
CPT utilizes an exposure component whereby the client accesses the traumatic memory via impact statements and recollections of the event, in a safe and empathic environment, leading to processing of emotions such as fear, anger, sadness, and guilt. CPT also focuses on how emotional responses to trauma impact one’s interpretation of the event. This part of therapy targets the content of cognitions, especially cognitive distortions, and how cognition impacts emotion and behavior. In an attempt to make sense of the traumatic event, individuals may assimilate, accommodate, or over-accommodate the experience into their world views. Assimilation involves fitting the event into one’s prior held beliefs. For example, if a client believes that good things happen to good people and bad things should happen to bad people, having a traumatic event occur may present conflicting information. Therefore, in order for the client to maintain their prior beliefs, they may blame themselves and assume they must have been bad in order for this bad thing to happen to them. Therapy would attempt to correct this attempt at assimilation. Over-accommodation is when the individual drastically changes his/her beliefs about the self and the world to achieve control and safety. The goal of the therapist is to assist the client in accommodation of the event in a healthy and balanced way (Resick, et al., 2008). The goal of therapy is to facilitate Accommodation, which is comprised of changing one’s beliefs enough to integrate the event in a healthy way. Treatment focuses on several areas that are thought to be most impacted by trauma: Safety, Trust, Power/Control, Esteem, Intimacy. Prolonged Exposure Therapy (PE): Treatment includes: psychoeducation about common reactions to trauma, breathing re-training, in-vivo exposures to situations or things that are being avoided by the client, and imaginal exposures to the client's traumatic memories. Emotion-Focused Therapy (EFT): Much like CPT recognizes the impact of emotion on trauma, EFT conceptualizes the transformation of emotion on a deepened level. It is a process-oriented approach that is influenced by its roots in Person-Centered, Gestalt, and Existential forms of therapy. The flexibility of EFT permits the implementation of other forms of therapy as supplemental tools, one of the many assets of this form of treatment. Emotional processing in this therapy allows for the gradual progression of emotion, and then as the arousal decreases, the emotion fades away. The individual expresses and reflects on the experience through language and symbolism, which sets the stage for emotional transformation. The exposure component of this type of therapy allows clients to overcome avoidance of emotion. When we simultaneously activate opposing emotions during session, we are able to “undo” old dysfunctional responses with more adaptive emotional experience (Greenberg, 2007). |
OakHeart PTSD Counselors, Psychologists, and Social Workers





PTSD Related Blogs:
|
Post-Traumatic Stress Disorder (PTSD) results from witnessing or being exposed to death, threatened death, or actual or threatened serious injury (American Psychiatric Association, 2013). Following such a terrifying event, our brains sometimes recover. Sometimes they do not. This is why PTSD is considered a recovery disorder (Resick et al., 2017). Symptoms include intrusive memories, efforts to avoid memories, increased negative emotions and thinking patterns, and hypervigilance or hyper-arousal (increased alertness and related physical symptoms). These are symptoms we all can experience after a traumatic event for a short period of time. However, PTSD occurs when these symptoms persist and start to impact your life, long term...(to read more, click on the link above).
|

|
Many of my patients who have been diagnosed with PTSD describe their traumatic memory as if the event just happened yesterday. They tell me it feels dangerous to examine the memory and to allow it into their minds. They tell me that any reminder of the memory also feels dangerous. This makes sense for a variety of reasons. First, thinking about the worst day or days of your life will understandably feel awful. Second, one component of PTSD is experiencing intrusive thoughts about the traumatic experience and other symptoms related to feelings of re-living the trauma, otherwise known as re-experiencing symptoms...(to read more, click on the link above).
|

|
A very common and natural response following any significant traumatic event and is one of the primary diagnostic criteria for posttraumatic stress disorder (PTSD) is hyperarousal, also known as hypervigilance. Biological changes in your mind and body which are initiated by a traumatic event instinctively remain alert to any additional potential threats to your wellbeing…both real or imagined. This is known as hypervigilance and can be an outcome of the anxiety experienced as part of Acute Stress Disorder or Posttraumatic Stress Disorder. The feelings of hypervigilance fluctuate and are often triggered by certain people or specific situations. Being in this constant state of heightened alert, tension, and “on guard” feeling for any hidden dangers is both stressful and exhausting to maintain over a prolonged period of time...(to read more, click on the link above).
|
Resources
References
Greenberg, L. S. (2007). A guide to conducting a task analysis of psychotherapeutic change. Psychotherapy Research, 17(1), p. 15-30.
Resick, P.A., Monson, C.M., & Chard, K.M. (2008). Cognitive processing therapy: Veteran/military version. Washington, DC: Department of Veterans’ Affairs.
Resick, P.A., Monson, C.M., & Chard, K.M. (2008). Cognitive processing therapy: Veteran/military version. Washington, DC: Department of Veterans’ Affairs.
